Decades of scientific effort and hundreds of billions of dollars have brought us to a strange, frustrating moment in medicine. We now have approved drugs that successfully clear toxic proteins from the brains of Alzheimer disease patients, yet these therapies do almost nothing to restore lost memories or stop the relentless march of cognitive decline. The medical establishment remains largely fixated on a single, flawed biological target, while alternative, highly promising avenues of research are starved of attention and funding. To truly solve the Alzheimer crisis, we must confront the uncomfortable truth that our current drug development model is fundamentally broken.
The primary culprit behind this stagnation is an industry-wide obsession with amyloid beta, the sticky protein plaque that accumulates in the brains of patients. For thirty years, the dominant theory held that removing these plaques would halt the disease. It did not. Newly approved monoclonal antibodies do indeed scrub the brain clean of amyloid, but the clinical benefit to patients is so microscopic that it is barely measurable in daily life. Meanwhile, patients face serious risks, including brain swelling and micro-hemorrhages. The science has moved on, but the money and the institutional momentum remain stubbornly left behind.
The Monoclonal Antibody Trap
Modern medicine loves a simple villain. For a generation, amyloid beta was cast in that role, leading to a gold rush among pharmaceutical giants seeking to develop the ultimate plaque-busting molecule.
The results of this narrow focus are now public record. Drugs like lecanemab and donanemab represent extraordinary triumphs of biochemical engineering, but their clinical utility is profoundly modest. In clinical trials, these therapies slowed cognitive decline by only about twenty-five to thirty percent over a year and a half. On an eighteen-point cognitive assessment scale, that translates to a difference of less than half a point between those who took the drug and those who took a placebo.
Most families would not even notice such a difference. They would, however, notice the safety risks.
About twenty percent of patients treated with these high-dose antibodies develop a condition known as Amyloid-Related Imaging Abnormalities, or ARIA. This condition manifests as localized brain swelling or small bleeds within the cerebral tissue. While many cases are asymptomatic and resolve on their own, some are severe, and a small number of patient deaths have been linked directly to the treatment.
We are asking patients and their families to accept a high risk of brain injury in exchange for a marginal delay in disease progression. This is a bad bargain. It is a bargain born of desperation, pushed by companies that need to recoup billions in research and development costs, and approved by regulators under immense public pressure to deliver something, anything, to a desperate population.
The Financial Inertia of a Failing Hypothesis
Why did the scientific community stay locked into the amyloid hypothesis for so long despite decades of failed clinical trials? The answer lies in the sociology of modern science and the economics of drug development.
Scientific research is not an objective, frictionless search for truth. It is an ecosystem governed by peer review, grant funding, and institutional prestige. Once the amyloid hypothesis gained dominance in the early 1990s, it created a self-reinforcing loop. The scientists who built their careers on amyloid became the reviewers who decided which papers got published and which grants got funded.
Dissent was quietly but effectively silenced. Researchers who suggested that amyloid might be a symptom rather than the cause of Alzheimer disease found themselves marginalized.
[Amyloid Hypothesis Dominates] ---> [Grants Awarded to Amyloid Projects]
^ |
| v
[Dissenting Theories Starved] <--- [Journals Publish Amyloid Papers]
This financial chokehold extended to the venture capital and pharmaceutical sectors. Developing a new drug from scratch costs upwards of one billion dollars. Boardrooms are notoriously risk-averse, preferring to fund projects that build on existing, well-trodden paths rather than betting on unproven biological mechanisms. Consequently, for three decades, almost every major clinical trial focused on different ways to attack the exact same target.
This is herd mentality on a global scale. The cost of this conformity is measured not just in wasted dollars, but in the millions of lives lost while alternative theories gathered dust on the shelves of underfunded university labs.
The True Culprits Inside the Aging Brain
To find therapies that actually work, we must look beyond the plaques. Alzheimer disease is not a simple, single-cause illness; it is a complex, systemic failure of the aging brain.
The Tangle of Tau
While amyloid accumulates outside of brain cells, another protein called tau forms destructive tangles inside the neurons themselves.
These tangles are far more dangerous than plaques. They disrupt the internal transport system of the neuron, cutting off the flow of nutrients and essential molecules. Eventually, the cell starves and dies. Crucially, the spread of tau tangles through the brain correlates directly with the severity of a patient's cognitive decline.
Where amyloid is present, cognitive symptoms may still be years away. When tau spreads, dementia is already actively destroying the mind. Therapies targeting tau are finally entering human trials, but they are years behind where they should be because they were ignored during the height of the amyloid gold rush.
The Fires of Neuroinflammation
The brain possesses its own dedicated immune system, primarily managed by specialized cells called microglia.
In a healthy brain, microglia act as vigilant housekeepers, clearing away debris, cellular waste, and even small amounts of amyloid. In the Alzheimer brain, however, this system malfunctions. The microglia become chronically hyperactive, releasing a continuous stream of inflammatory chemicals that damage nearby neurons instead of protecting them.
The brain essentially sets itself on fire. This chronic neuroinflammation is not a side effect of the disease; it is a primary driver of its progression. Finding ways to calm these overactive immune cells without leaving the brain vulnerable to infections is one of the most promising frontiers in neurology today.
Metabolic Collapse and Type 3 Diabetes
The human brain is an energy hog, consuming roughly twenty percent of the body's glucose despite representing only two percent of its weight.
In many Alzheimer patients, the brain loses its ability to harvest energy from glucose effectively. This localized insulin resistance has led some prominent researchers to refer to Alzheimer disease as Type 3 diabetes. When brain cells cannot get the fuel they need, they begin to wither and lose their connections.
If we cannot restore energy production to these starving cells, no amount of plaque removal will keep them alive. Therapies aimed at improving brain metabolism, including repurposing existing diabetes medications, represent a cheap and logical approach that has been systematically undervalued by major pharmaceutical developers looking for high-margin, proprietary biologics.
The Nightmare of Clinical Trial Design
Even when a researcher identifies a brilliant new drug target, getting that drug through the regulatory pipeline is an administrative and financial nightmare.
The biggest hurdle is timing. Alzheimer disease begins silently. Damage to the brain starts occurring twenty to thirty years before a patient forgets where they put their keys or struggles to find the right word.
By the time a patient qualifies for a clinical trial because of mild cognitive impairment, they have already lost millions of critical synapses. Attempting to cure them at this stage is like trying to put out a forest fire after half the trees have already burned to ash.
To test preventive drugs, researchers need to run trials that last five, ten, or fifteen years.
No pharmaceutical company wants to fund a fifteen-year trial. The patent on the drug would expire shortly after the trial concluded, leaving the company with no way to claw back its investment. We are trapped in a system where the business model of medicine directly conflicts with the biology of the disease.
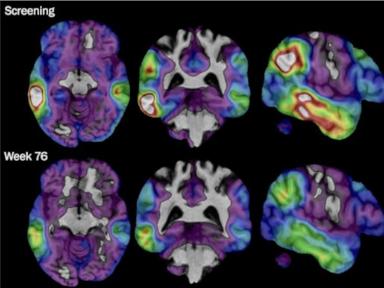
Furthermore, we lack reliable, cheap biomarkers for these newer targets. We can easily visualize amyloid plaques using expensive PET scans, which makes it easy to show regulators that a drug is doing something. We do not yet have equally clear, widely accepted ways to measure real-time changes in neuroinflammation or synaptic health. Without those tools, running a clean, persuasive clinical trial for a non-amyloid drug is incredibly difficult.
The Fallacy of the Single Pill
We must abandon the fantasy of the magic bullet.
There will never be a single pill that cures Alzheimer disease. The pathology is too complex, involving a cascading failure of proteins, blood vessels, immune responses, and metabolic pathways. Expecting a single drug to cure Alzheimer is like expecting a single mechanic to fix a car that has a dead battery, a broken transmission, and a punctured fuel tank all at once.
Instead, the future lies in combination therapies. We must learn from our successes in other fields of medicine.
We do not treat HIV with a single drug; we use a cocktail of multiple compounds that attack the virus at different stages of its life cycle. We do not treat complex cancers with a single agent; we combine chemotherapy, immunotherapy, and targeted molecular therapies to overwhelm the disease from multiple angles.
Alzheimer disease requires the exact same approach. A patient may need one drug to calm neuroinflammation, another to stabilize tau proteins, a third to boost brain metabolism, and perhaps a fourth to clear away amyloid.
Our current regulatory and commercial frameworks are entirely unprepared for this reality. Drug companies are highly reluctant to test their experimental compounds in combination with a competitor's experimental drug due to liability, patent sharing, and intellectual property disputes. The FDA is set up to approve single agents, not complex, multi-company cocktails.
Until we restructure our clinical trial networks and build regulatory pathways specifically designed to evaluate combination therapies, we will continue to watch promising molecules fail in isolation. The science is ready for a multidimensional attack on dementia. The system that funds and regulates that science is not.



